
Introduction
Acute Kidney Injury (AKI) is a sudden decline in kidney function that develops over hours to days. The kidneys play a vital role in filtering waste products, balancing electrolytes, regulating fluid levels, and maintaining acid–base balance in the body. When they abruptly lose this ability, harmful substances accumulate in the bloodstream, potentially leading to life-threatening complications if not recognized early.
Previously referred to as “acute renal failure,” AKI is now the preferred term because kidney damage can range from mild dysfunction to complete failure. Importantly, AKI is often reversible if diagnosed and treated promptly. However, delayed recognition may result in long-term kidney damage or progression to chronic kidney disease.
About Acute Kidney Injury (AKI)
Acute Kidney Injury refers to a rapid deterioration in kidney function, characterized by a rise in serum creatinine and/or a decrease in urine output. Unlike chronic kidney disease, which progresses gradually over months or years, AKI develops suddenly.
The kidneys normally filter about 180 liters of blood daily. They remove waste such as urea and creatinine, regulate sodium and potassium levels, control blood pressure through hormonal mechanisms, and maintain fluid balance. In AKI, this filtering process becomes impaired.
AKI can occur in hospitalized patients, especially those in intensive care units, but it can also develop in the community due to dehydration, infections, or medication-related causes.
Signs and Symptoms
The presentation of AKI varies depending on severity and underlying cause. Some patients may have subtle symptoms, while others develop severe complications.
Common Symptoms
- Reduced urine output (though some patients may have normal urine volume)
- Swelling in legs, ankles, or around the eyes
- Fatigue and weakness
- Nausea or vomiting
- Shortness of breath
- Confusion or drowsiness
- Chest discomfort (if fluid accumulates around the heart)
Warning Signs of Severe AKI
- Very little or no urine
- Irregular heartbeat due to electrolyte imbalance
- Seizures
- Severe breathlessness due to fluid overload
Because early symptoms may be mild, routine blood tests often detect AKI before symptoms become obvious.
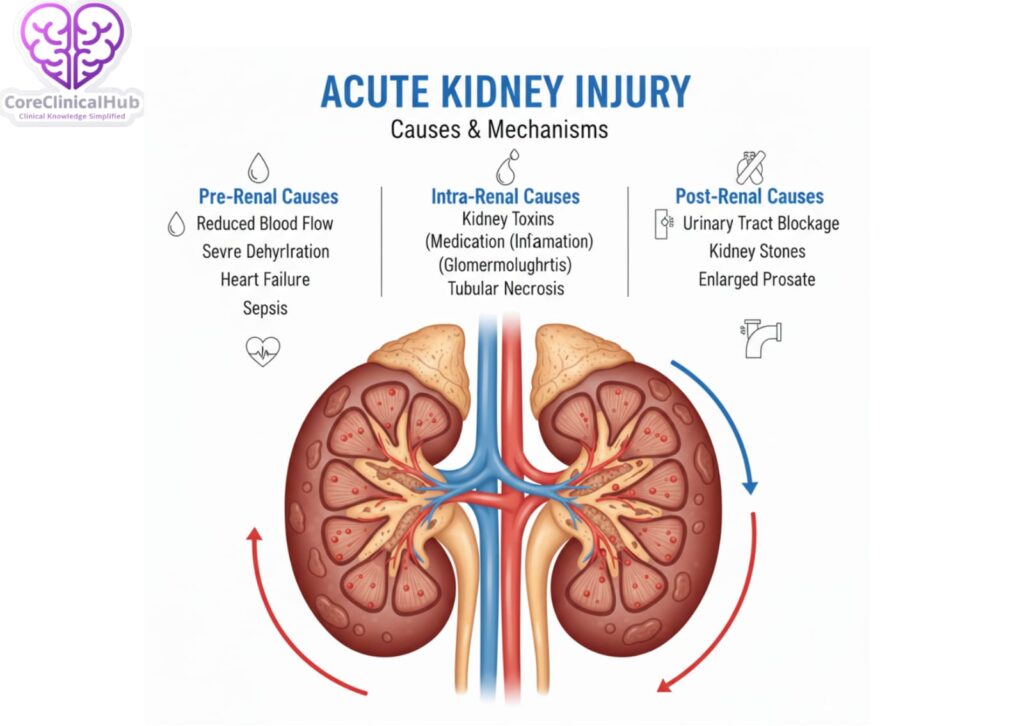
Causes
AKI is broadly classified into three categories based on the underlying mechanism:
1. Pre-renal Causes (Reduced Blood Flow to Kidneys)
These occur when there is inadequate blood supply to the kidneys.
- Severe dehydration
- Blood loss
- Heart failure
- Severe infections (sepsis)
- Low blood pressure
- Burns
2. Intrinsic (Intrinsic Renal) Causes
These involve direct damage to kidney tissues.
- Acute tubular necrosis (commonly due to prolonged low blood flow or toxins)
- Glomerulonephritis
- Acute interstitial nephritis (often medication-induced)
- Certain antibiotics and painkillers
- Contrast dye used in imaging studies
3. Post-renal Causes (Obstruction)
These result from blockage in urine outflow.
- Kidney stones
- Enlarged prostate
- Tumors compressing urinary tract
- Blood clots in urinary passages
Identifying the category is essential because treatment depends heavily on the cause.
Risk Factors
Certain individuals are more vulnerable to developing AKI:
- Advanced age
- Diabetes mellitus
- High blood pressure
- Pre-existing chronic kidney disease
- Heart disease
- Liver disease
- Severe infections
- Major surgery
- Use of nephrotoxic medications (e.g., NSAIDs, some antibiotics)
- Dehydration
- Prolonged ICU stay
Recognizing high-risk patients allows preventive strategies to be implemented early.
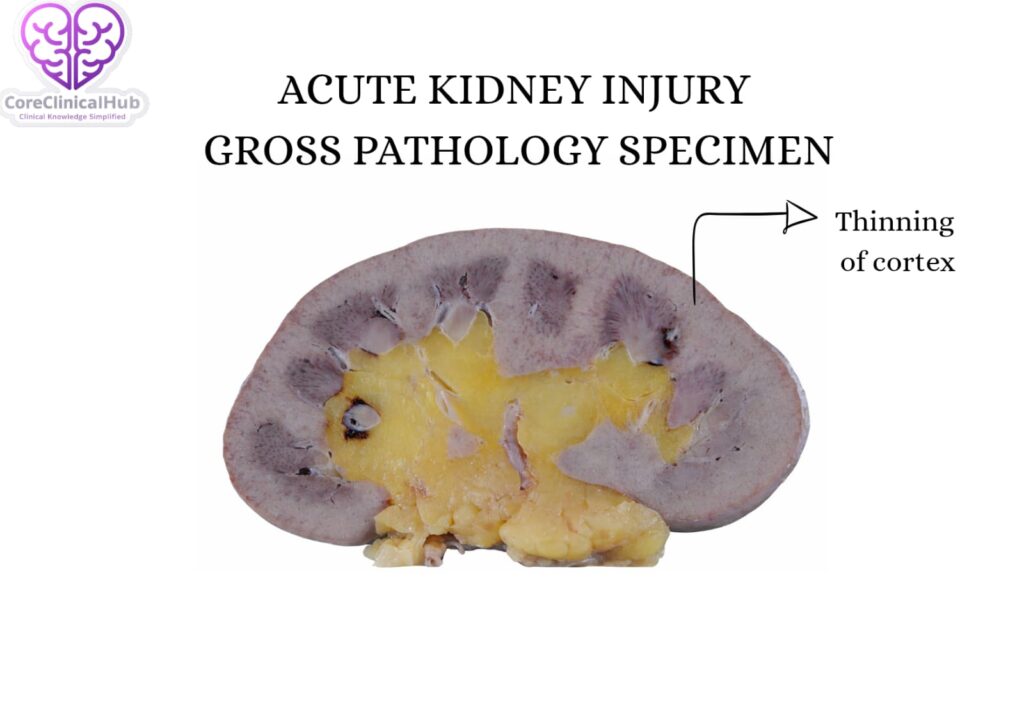
Pathophysiology (How AKI Develops)
The mechanisms behind AKI differ depending on the cause, but several processes commonly occur:
- Reduced oxygen delivery to kidney tissues
- Direct injury to tubular cells
- Inflammatory responses within kidney structures
- Obstruction of urine flow
- Impaired filtration at the glomerulus
When kidney cells are deprived of oxygen or exposed to toxins, they become damaged. Tubular cells may swell, detach, and block normal urine flow. Inflammatory mediators further worsen the injury.
If blood flow is restored quickly, many kidney cells can recover. However, prolonged injury may result in permanent scarring.
Complications
If untreated or severe, AKI can lead to serious complications:
- Fluid overload leading to pulmonary edema
- Hyperkalemia (high potassium levels) causing dangerous heart rhythms
- Metabolic acidosis
- Uremia (accumulation of waste products)
- Pericarditis
- Sepsis
- Progression to chronic kidney disease
- Need for long-term dialysis
Early recognition significantly reduces the risk of these complications.
Diagnosis
Clinical Evaluation
A thorough medical history is essential. Important points include:
- Recent illness or infection
- Medication use
- Fluid intake
- History of kidney disease
Laboratory Tests
- Serum creatinine: A sudden rise indicates reduced kidney function.
- Blood urea nitrogen (BUN)
- Electrolytes: Especially potassium levels.
- Urine analysis: To check for protein, blood, or casts.
- Urine output monitoring
Imaging
- Ultrasound to detect obstruction
- CT scan if stones or masses are suspected
Diagnostic Criteria
AKI is generally diagnosed when one of the following occurs:
- Increase in serum creatinine by ≥0.3 mg/dL within 48 hours
- Increase in serum creatinine to ≥1.5 times baseline within 7 days
- Urine output less than 0.5 mL/kg/hour for 6 hours
Staging of AKI
AKI is classified into stages (Stage 1, 2, and 3) based on severity of creatinine elevation and urine output reduction. Higher stages indicate more severe injury and worse prognosis.
Treatment
Management of AKI depends on identifying and correcting the underlying cause.
1. Correcting Pre-renal Causes
- Intravenous fluids for dehydration
- Blood transfusion if significant blood loss
- Treating heart failure
- Managing sepsis
2. Addressing Intrinsic Causes
- Discontinuing nephrotoxic drugs
- Treating infections
- Steroids in selected inflammatory conditions
3. Relieving Obstruction
- Catheterization
- Stent placement
- Surgical removal of stones or tumors
4. Supportive Care
- Strict fluid balance monitoring
- Electrolyte correction
- Avoiding further kidney toxins
- Adjusting medication dosages
5. Dialysis
Temporary dialysis may be required in cases of:
- Severe hyperkalemia
- Fluid overload unresponsive to treatment
- Severe metabolic acidosis
- Uremic complications
Dialysis supports the body while kidneys recover.
Diet in Acute Kidney Injury
Nutrition plays an important supportive role during AKI.
General Dietary Principles
- Moderate protein intake (not excessive)
- Restrict potassium if levels are high
- Limit sodium to prevent fluid retention
- Control phosphorus intake
- Adequate calories to prevent muscle breakdown
Foods to Monitor
- High potassium foods: bananas, oranges, tomatoes
- Processed foods high in sodium
- High phosphorus foods: cola drinks, processed cheese
A dietitian’s guidance is beneficial, especially in hospitalized patients.
Prevention Strategies
AKI is often preventable, especially in high-risk individuals.
- Maintain adequate hydration
- Avoid unnecessary NSAIDs
- Monitor kidney function during serious illness
- Adjust drug dosages in elderly patients
- Monitor kidney function after contrast imaging
- Early treatment of infections
- Proper blood pressure and diabetes control
Hospital protocols now emphasize early detection through regular monitoring of urine output and creatinine levels.
Preparing for Your Appointment
If you suspect kidney problems or have been diagnosed with AKI, preparation helps improve consultation quality.
Before Visiting the Doctor:
- List all medications (including over-the-counter drugs)
- Note recent illnesses or hospitalizations
- Track urine output if possible
- Document symptoms and their duration
Questions You May Ask:
- What caused my AKI?
- Is it reversible?
- Will I need dialysis?
- What lifestyle changes are required?
- How often should kidney function be monitored?
Prognosis
The outcome of AKI depends on:
- Severity
- Underlying cause
- Timeliness of treatment
- Presence of other illnesses
Many patients recover completely within weeks. However, some may develop residual kidney damage, increasing future risk of chronic kidney disease.
Long-term follow-up is recommended even after apparent recovery.
Long-Term Monitoring
After recovery:
- Periodic serum creatinine testing
- Blood pressure control
- Monitoring urine protein
- Lifestyle modifications
Patients who experienced severe AKI should undergo regular kidney assessments for at least 6–12 months.
References
- International clinical practice guidelines for acute kidney injury.
- Current nephrology consensus recommendations on AKI management.
- Standard internal medicine reference texts on renal physiology and pathology.
- Recent peer-reviewed nephrology journals discussing AKI outcomes.
Frequently Asked Questions (FAQs)
Is Acute Kidney Injury reversible?
Yes, many cases are reversible if treated early, especially pre-renal causes like dehydration.
How quickly does AKI develop?
It can develop within hours to days depending on the trigger.
Can dehydration alone cause AKI?
Yes, severe dehydration can significantly reduce blood flow to the kidneys and trigger AKI.
Is dialysis permanent in AKI?
Usually not. Dialysis in AKI is often temporary until kidney function recovers.
What is the difference between AKI and chronic kidney disease?
AKI develops suddenly and may be reversible, whereas chronic kidney disease progresses slowly and is usually permanent.
Can medications cause AKI?
Yes, certain antibiotics, NSAIDs, contrast agents, and chemotherapy drugs may cause kidney injury.
How is urine output related to AKI?
Reduced urine output is an important diagnostic criterion and severity marker.
Can AKI occur without symptoms?
Yes, especially in early stages. Blood tests often detect it before symptoms appear.
Who is most at risk for AKI?
Elderly individuals, diabetics, heart disease patients, and hospitalized critically ill patients.
How can I prevent AKI during illness?
Stay hydrated, avoid unnecessary painkillers, monitor kidney function if high-risk, and seek medical care early.