
Hyperkalemia is a potentially life-threatening electrolyte emergency that can cause fatal cardiac arrhythmias if not recognized early.
Potassium is predominantly an intracellular cation. Total body potassium stores range from 50 to 75 mEq/kg body weight, corresponding to approximately 3,000 mEq.
- Serum potassium > 5.5 mEq/L is defined as hyperkalemia.
Normal Serum potassium: 3.5 – 5.0 mEq/L
Why Hyperkalemia Is Dangerous?
Potassium plays a key role in:
- Resting membrane potential
- Neuromuscular transmission
- Cardiac conduction
Hyperkalemia disturbs the resting membrane potential of excitable cells, particularly cardiac myocytes, predisposing to life-threatening arrhythmias, conduction abnormalities, and neuromuscular manifestations, including muscle weakness or paralysis.
Stepwise Clinical Approach to Hyperkalemia
STEP 1: Confirm It’s True Hyperkalemia
Always rule out pseudohyperkalemia
The most common apparent cause of hyperkalemia is pseudohyperkalemia, which does not reflect true serum potassium concentrations. Pseudohyperkalemia frequently results from hemolysis during specimen collection, releasing intracellular potassium into the serum
Causes of Pseudohyperkalemia:
- Hemolyzed blood sample
- Prolonged tourniquet use
- Thrombocytosis
- Severe leukocytosis
👉 Repeat serum potassium if suspicion exists.
STEP 2: Assess Severity
| Potassium Level | Severity |
| 5.5 – 6.0 | mild |
| 6.9 – 6.9 | moderate |
| >7.0 | severe [Emergency] |
⚠️ But remember: ECG changes matter more than number
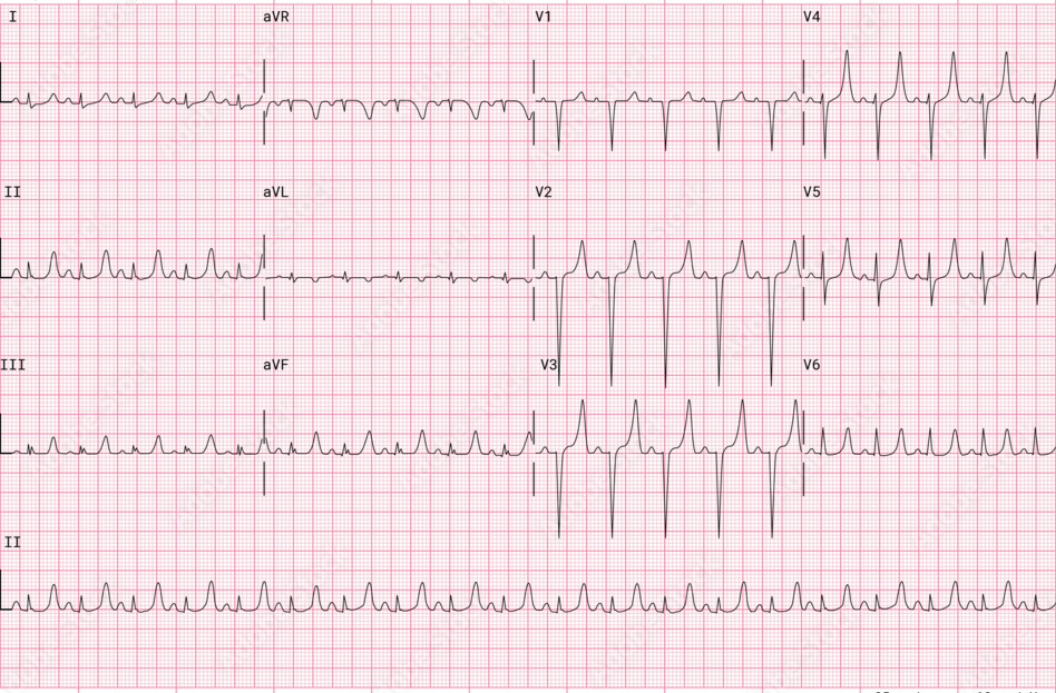
STEP 3: Look for ECG Changes
Progressive ECG Changes in Hyperkalemia:
- Peaked T waves (tall, tented)
- PR prolongation
- P wave flattening
- QRS widening
- Sine wave pattern
- Ventricular fibrillation / Asystole
💡 Exam Pearl:
- Peaked T waves are the earliest ECG sign.
Causes of Hyperkalemia (Exam-Oriented Classification)
1️⃣ Decreased Excretion (Most Common)
- Acute kidney injury
- Chronic kidney disease
- Hypoaldosteronism
- Type 4 RTA
- Addison’s disease
2️⃣ Shift from ICF to ECF
- Metabolic acidosis
- Insulin deficiency (DKA)
- Beta-blockers
- Succinylcholine
- Tumor lysis syndrome
- Rhabdomyolysis
3️⃣ Increased Intake (Rare Alone)
- Excess potassium supplements
- Massive blood transfusion
Important Cause: Type 4 RTA
Seen in:
- Diabetics
- CKD patients
- Patients on ACE inhibitors / ARBs
Mechanism: Low aldosterone → decreased K+ excretion → hyperkalemia
Clinical Features
Often asymptomatic until severe.
Symptoms:
- Muscle weakness
- Paresthesia
- Flaccid paralysis
- Cardiac arrhythmias
ECG Changes in Hyperkalemia (Stepwise Progression)
Hyperkalemia produces predictable, progressive ECG changes as serum potassium rises.
⚠️ Important:
ECG severity does not always correlate exactly with potassium level. Some patients may develop severe changes at relatively lower values.
Why Does Hyperkalemia Affect ECG?
Potassium controls the resting membrane potential of cardiac myocytes.
↑ Extracellular potassium →↓ Membrane excitability →Slowed conduction →Life-threatening arrhythmias
Progressive ECG Changes in Hyperkalemia
1️⃣ Peaked (Tented) T Waves – Earliest Sign
Serum K⁺: ~5.5–6.5 mEq/L
ECG Features:
- Tall, narrow, symmetrical T waves
- Best seen in precordial leads (V2–V4)
- Shortened QT interval
💡 Important Pearl:
Peaked T wave is the earliest ECG change in hyperkalemia.

2️⃣ PR Prolongation & P Wave Flattening
Serum K⁺: ~6.0–7.0 mEq/L
ECG Features :
- Prolonged PR interval
- Decreased P wave amplitude
- T waves remain peaked
Mechanism :
Atrial conduction slows first.
3️⃣ P Wave Disappearance & QRS Widening
Serum K⁺: ~7.0–8.0 mEq/L
ECG Features :
- P waves disappear
- QRS complex widens
- Conduction delays
- T waves still tall
⚠️ This is a dangerous stage.
4️⃣ Sine Wave Pattern – Pre-Arrest Stage
Serum K⁺: >8.0 mEq/L
ECG Features :
- QRS merges with T wave
- Smooth sine-wave appearance
- No P waves
- Extreme QRS widening
⚠️ This precedes:
- Ventricular fibrillation
- Asystole
- Cardiac arrest
Visual Summary Table
| Potassium Level | ECG Change | Clinical Danger |
| 5.5 – 6.5 | Peaked T waves | Early |
| 6.0 – 7.0 | PR Prolongation | Moderate |
| 7.0 – 8.0 | Wide QRS | Severe |
| >8.0 | Sine wave | Cardiac arrest |
Important Pearls
- Earliest ECG change → Peaked T wave
- Most dangerous pattern → Sine wave
- First drug if ECG changes present → IV Calcium gluconate
- Hyperkalemia can cause bradycardia
- Can mimic STEMI due to tall T waves
Emergency Management of Hyperkalemia (Stepwise Protocol)
⚠️ Treat immediately if:
- K+ ≥ 6.5
- ECG changes present
Initial management involves immediate discontinuation of exogenous potassium sources and concurrent treatment of any reversible underlying cause.
Step 1: Stabilize Cardiac Membrane
IV Calcium Gluconate
- 10 mL of 10% solution IV over 2–5 minutes
✔️ Does NOT lower potassium
✔️ Protects heart
Step 2: Shift Potassium into Cells
1. Insulin + Dextrose
10 units regular insulin IV
25 g glucose
Effect in 15–30 minutes
2. Beta-2 Agonist
Salbutamol Nebulization
3. Sodium Bicarbonate
Useful if metabolic acidosis present
Step 3: Remove Potassium from Body
1. Loop Diuretics
2. Potassium binders
- Sodium polystyrene sulfonate
- Patiromer
3. Hemodialysis (Definitive Treatment)
Indicated in:
- Severe hyperkalemia
- Renal failure
- Refractory cases
Management Summary Table
| Step | Drug | Action |
| 1 | Calcium gluconate | Stabilizes myocardium |
| 2 | Insulin + glucose | Shifts K+ into cells |
| 3 | Beta agonist | Shifts K+ into cells |
| 4 | Dialysis | Removes K+ Permanently |
Hyperkalemia in Special Conditions
DKA
Initial potassium may be high
But total body potassium is low
⚠️ Always monitor during insulin therapy
Tumor Lysis Syndrome
Massive cell breakdown → sudden potassium release
When to Admit?
Admit if:
- K+ > 6.0
- ECG changes
- Renal failure
- Symptomatic patient
Prevention Tips
- Monitor potassium in CKD
- Caution with ACE inhibitors
- Avoid potassium-rich diet in renal failure