
Introduction
Hypokalemia refers to a serum potassium level below 3.5 mEq/L. Potassium is the most important intracellular cation and plays a critical role in maintaining resting membrane potential, neuromuscular function, and cardiac conduction.
Symptoms may include feeling tired , leg cramps , weakness and constipation
Even mild reductions in potassium can cause significant cardiac and neuromuscular disturbances. Severe hypokalemia may lead to life-threatening arrhythmias and respiratory muscle paralysis.
Normal Potassium Physiology
- Normal serum potassium: 3.5–5.0 mEq/L
- 98% of potassium is intracellular
- Maintained by :
- Na⁺/K⁺ ATPase pump
- Renal regulation
- Acid-base balance
- Hormonal control (especially aldosterone and insulin)
Small changes in extracellular potassium can significantly affect cardiac excitability.
Classification of Hypokalemia
| Severity | Serum Potassium |
| Mild | 3.0 – 3.5 mEq/L |
| Moderate | 2.5 – 3.0 mEq/L |
| Severe | <2.5 mEq/L |
Severe Hypokalemia requires urgent evaluation and monitoring.
Causes of Hypokalemia
Hypokalemia occurs due to :
- Decreased intake
- Shift of potassium into cells
- Increased potassium loss
1️⃣ Decreased Intake (Rare Alone)
- Starvation
- Eating disorders
- Poor nutritional intake
Usually contributes along with other causes.
2️⃣ Transcellular Shift (Potassium Moves Into Cells)
Potassium shifts intracellularly in:
- Alkalosis
- Insulin administration
- Beta-agonists (e.g., salbutamol)
- Periodic paralysis (familial or thyrotoxic)
📌 Clue: No total body potassium deficit, only redistribution.
3️⃣ Increased Potassium Loss (Most Common Cause)
A. Renal Loss
- Diuretics (loop, thiazide)
- Hyperaldosteronism
- Cushing syndrome
- Renal tubular disorders:
- Bartter syndrome
- Gitelman syndrome
- Renal tubular acidosis (Type 1 & 2)
- Hypomagnesemia
📌 Check urine potassium to differentiate renal from extrarenal loss.
B. Gastrointestinal Loss
- Vomiting
- Diarrhea
- Laxative abuse
- Nasogastric suction
📌 Vomiting causes metabolic alkalosis and secondary renal potassium loss.
Stepwise Clinical Approach to Hypokalemia
Step 1: Confirm the Potassium Level
- Rule out lab error
- Repeat test if needed
- Check for hemolysis (which falsely elevates potassium, not lowers)
Step 2: Assess Severity & Symptoms
Look for:
Neuromuscular Symptoms
- Muscle weakness
- Cramps
- Fatigue
- Paralysis (ascending)
- Hyporeflexia
Gastrointestinal
- Constipation
- Ileus
Cardiac
- Palpitations
- Arrhythmias
Severe hypokalemia can cause respiratory muscle weakness.
Step 3: Look for ECG Changes
ECG findings are progressive:
- Flattened T waves
- ST depression
- Prominent U waves
- Prolonged QU interval
- Ventricular arrhythmias (in severe cases)
📌 Presence of U wave is a classic exam finding.
Step 4: Determine the Cause
Check Urine Potassium
- Urine K < 20 mEq/L → Extrarenal loss (GI causes)
- Urine K > 20 mEq/L → Renal loss
Further evaluation :
- Check blood pressure
- Check acid-base status
- Measure magnesium levels
Acid-Base Based Approach
Hypokalemia + Metabolic Alkalosis
- Vomiting
- Diuretics
- Hyperaldosteronism
- Bartter/Gitelman
Hypokalemia + Metabolic Acidosis
- Diarrhea
- Renal tubular acidosis
Hypokalemia and Magnesium Relationship
Hypomagnesemia causes:
- Persistent hypokalemia
- Refractory to potassium correction
📌 Always correct magnesium first.
Mechanism: Magnesium deficiency increases renal potassium wasting.
Clinical Features of Hypokalemia
Neuromuscular Effects
- Muscle weakness (proximal > distal)
- Cramps
- Paralysis
- Rhabdomyolysis (rare but serious)
- Severe cases may resemble Guillain-Barré.
Cardiac Effects
Hypokalemia increases cardiac excitability and risk of:
- Ventricular tachycardia
- Torsades de pointes
- Premature ventricular contractions
- Digitalis toxicity
- Patients on digoxin are at higher risk.
Renal Effects
- Polyuria
- Polydipsia
- Nephrogenic diabetes insipidus (chronic cases)
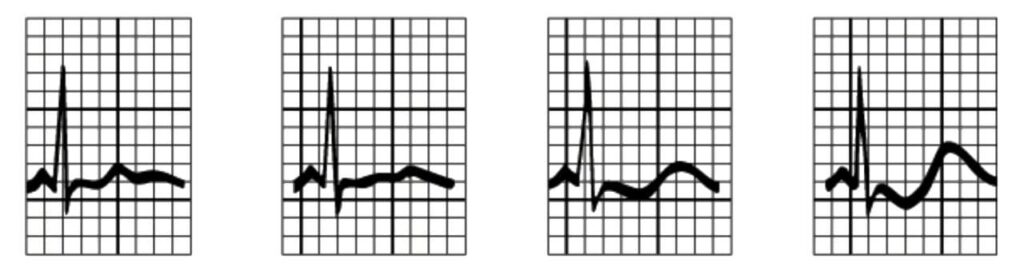
ECG Changes in Hypokalemia
Typical ECG progression:
- Decreased T wave amplitude
- ST segment depression
- Appearance of U wave (after T wave)
- T and U wave fusion
- Ventricular arrhythmias
📌 The QU interval prolongs (not true QT).
Special Conditions Associated with Hypokalemia
1️⃣ Periodic Paralysis
- Familial
- Thyrotoxic periodic paralysis
Episodes of muscle weakness with low potassium.
2️⃣ Diuretic-Induced Hypokalemia
- Loop and thiazide diuretics increase distal sodium delivery → increased potassium secretion.
3️⃣ Hyperaldosteronism
- Hypertension
- Hypokalemia
- Metabolic alkalosis
Classic triad.
Complications of Hypokalemia
- Cardiac arrhythmias
- Respiratory muscle paralysis
- Rhabdomyolysis
- Sudden cardiac death
Severity correlates with rate of fall rather than absolute value.
Management of Hypokalemia
Treatment depends on severity and symptoms.
1️⃣ Mild (3.0–3.5 mEq/L)
- Oral potassium supplements
- Dietary potassium increase
- Banana
- Coconut water
- Spinach
- Avocado
2️⃣ Moderate (2.5–3.0 mEq/L)
- Oral potassium preferred
- Monitor ECG if symptomatic
3️⃣ Severe (<2.5 mEq/L or symptomatic)
- IV potassium chloride
- Continuous cardiac monitoring
- Correct magnesium deficiency
IV Potassium Rules
- Maximum peripheral infusion rate: 10 mEq/hour
- Central line: up to 20 mEq/hour (with monitoring)
- Never give IV push
- Always dilute properly
Rapid correction can cause arrhythmias.
How Much Potassium is Needed?
Approximate rule:
1 mEq/L decrease ≈ 100–200 mEq total body deficit
This varies based on patient factors.
Prevention Strategies
- Monitor electrolytes in:
- Diuretic therapy
- ICU patients
- Insulin therapy
- Treat underlying cause
- Correct magnesium deficiency
Hypokalemia vs Hyperkalemia (Quick Contrast)
| Feature | Hypokalemia | Hyperkalemia |
| T wave | Flattened | Peaked |
| U wave | Present | Absent |
| Muscle effect | Weakness | Weakness |
| Arrhythmia risk | Yes | Yes |
Conclusion
Hypokalemia is a common yet potentially life-threatening electrolyte disorder. A structured approach helps in rapid diagnosis and management:
- Confirm potassium level
- Assess severity
- Check ECG
- Determine renal vs extrarenal loss
- Correct potassium safely
Early recognition prevents fatal arrhythmias and complications.