
Introduction
Nephrotic syndrome is a clinical condition that arises when the kidneys lose their ability to properly filter blood, leading to excessive loss of protein in the urine. Rather than being a single disease, it is a group of signs and symptoms that reflect damage to the filtering units of the kidneys, known as glomeruli.
This condition can affect children and adults, and its severity may range from mild swelling to life-threatening complications if not addressed early. Understanding the mechanisms, causes, diagnostic criteria, and management strategies is essential for both healthcare professionals and patients.
Understanding Kidney Function and Glomeruli
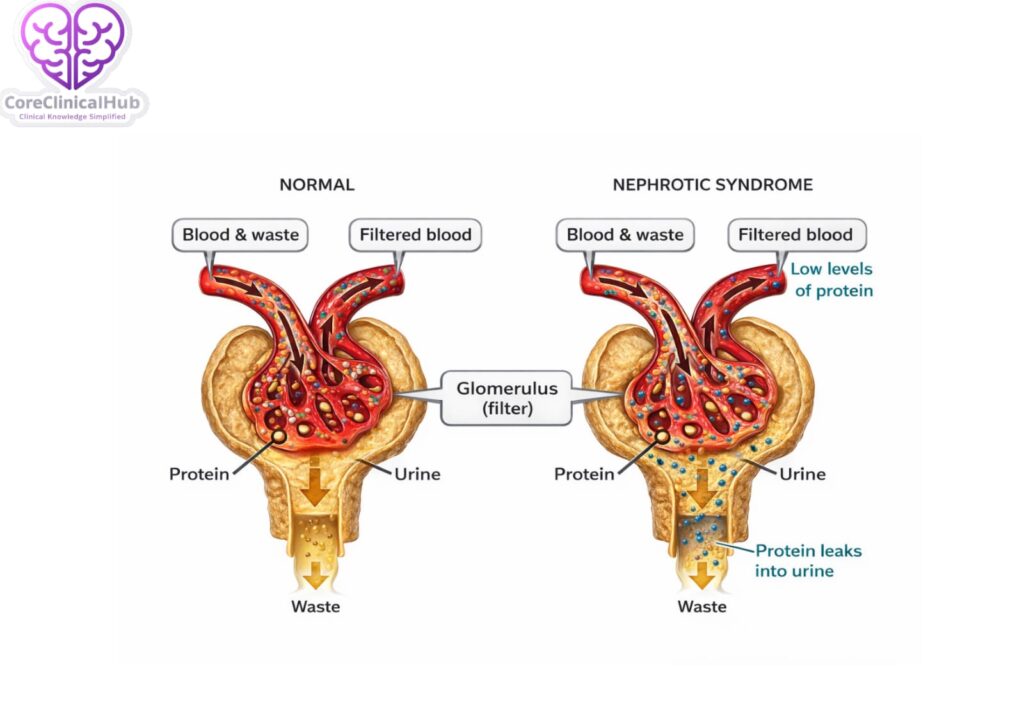
To appreciate nephrotic syndrome, it is important to understand how healthy kidneys work. Each kidney contains approximately one million filtering units called glomeruli. These microscopic structures act as sieves, allowing waste products and excess fluid to pass into urine while retaining essential substances like proteins and blood cells.
One of the most important proteins retained in the bloodstream is albumin. Albumin helps maintain oncotic pressure, which prevents fluid from leaking out of blood vessels into surrounding tissues. When glomeruli are damaged, they become abnormally permeable, allowing proteins to leak into the urine — a process known as proteinuria.
What is Nephrotic Syndrome?
Nephrotic syndrome is defined by a characteristic combination of:
- Heavy proteinuria (usually >3.5 grams per day in adults)
- Hypoalbuminemia (low blood albumin levels)
- Edema (swelling)
- Hyperlipidemia (elevated blood lipids)
- Lipiduria (fat in urine)
These features occur because of structural or functional damage to the glomerular filtration barrier.
Pathophysiology: What Happens Inside the Kidney?
The glomerular filtration barrier consists of three layers:
- Endothelial cells
- Basement membrane
- Podocytes (specialized epithelial cells)
Damage to any of these layers increases permeability to plasma proteins. The loss of albumin into urine reduces plasma oncotic pressure, leading to fluid movement from blood vessels into tissues, resulting in edema.
The liver compensates for low albumin levels by increasing protein synthesis. However, it also increases lipoprotein production, causing hyperlipidemia. Reduced protein levels may also lead to increased clotting tendency and weakened immunity.
Causes of Nephrotic Syndrome
Nephrotic syndrome can be broadly classified into primary and secondary causes.
1. Primary (Idiopathic) Causes
These originate within the kidney itself:
- Minimal Change Disease (common in children)
- Focal Segmental Glomerulosclerosis (FSGS)
- Membranous Nephropathy
- Membranoproliferative Glomerulonephritis
2. Secondary Causes
These occur due to systemic diseases:
- Diabetes mellitus
- Systemic lupus erythematosus
- Infections (hepatitis B, hepatitis C, HIV)
- Certain medications (NSAIDs, some antibiotics)
- Malignancies
- Amyloidosis
Identifying the underlying cause is crucial because treatment depends heavily on etiology.
Risk Factors
Certain factors increase the likelihood of developing nephrotic syndrome:
- Poorly controlled diabetes
- Autoimmune disorders
- Chronic infections
- Long-term use of nephrotoxic drugs
- Family history of kidney diseases
- Exposure to toxins
- Obesity and metabolic syndrome
Early screening in high-risk individuals can help prevent complications.
Clinical Features
1. Edema
Swelling is the most prominent symptom. It commonly starts around the eyes (periorbital edema) and later affects the legs, abdomen (ascites), and even genital region. Severe cases may result in generalized swelling (anasarca).
2. Frothy Urine
Excess protein in urine creates bubbles or foam.
3. Weight Gain
Rapid weight gain due to fluid accumulation.
4. Fatigue
Loss of protein may cause weakness and tiredness.
5. Decreased Urine Output
In some cases, urine production may decrease.
Diagnostic Criteria
Nephrotic syndrome is diagnosed based on laboratory and clinical findings.
Essential Diagnostic Features:
- Proteinuria >3.5 g/day (adults) or urine protein/creatinine ratio in spot sample
- Serum albumin <3.0 g/dL
- Edema
- Elevated serum cholesterol and triglycerides
Investigations
- Urine Routine Examination – Detects protein and lipid bodies
- 24-hour Urine Protein Estimation
- Serum Albumin and Total Protein
- Lipid Profile
- Renal Function Tests (Creatinine, Blood Urea)
- Blood Sugar Levels
- Autoimmune Markers (ANA, complement levels)
- Viral Markers
- Kidney Ultrasound
- Kidney Biopsy (if required to determine cause)
Kidney biopsy is often essential in adults to identify the specific pathological type.
Complications of Nephrotic Syndrome
If untreated or poorly controlled, nephrotic syndrome may lead to serious complications:
1. Infections
Loss of immunoglobulins increases susceptibility to infections, particularly pneumonia and peritonitis.
2. Thromboembolism
Protein loss includes anticoagulant factors, increasing the risk of blood clots such as deep vein thrombosis or pulmonary embolism.
3. Acute Kidney Injury
Severe cases may impair kidney function.
4. Chronic Kidney Disease
Long-standing glomerular damage may progress to irreversible kidney failure.
5. Malnutrition
Loss of protein can cause muscle wasting and weakness.
Management of Nephrotic Syndrome
Management includes treating the underlying cause and controlling symptoms.
1. General Measures
- Salt restriction to reduce edema
- Fluid restriction in severe cases
- Daily weight monitoring
- Blood pressure control
2. Medications
a) Corticosteroids
Commonly used in minimal change disease and some primary conditions.
b) Immunosuppressive Agents
Cyclophosphamide, tacrolimus, or mycophenolate in steroid-resistant cases.
c) ACE Inhibitors / ARBs
Reduce proteinuria and protect kidney function.
d) Diuretics
Help relieve swelling by removing excess fluid.
e) Statins
Manage hyperlipidemia.
f) Anticoagulants
Used in high-risk patients for clot prevention.
3. Treatment of Secondary Causes
- Tight glucose control in diabetes
- Immunotherapy in lupus
- Antiviral treatment in viral infections
- Discontinuation of offending drugs
Diet in Nephrotic Syndrome
Diet plays a significant supportive role.
Protein Intake
Moderate protein intake is recommended. Excess protein may worsen proteinuria, while very low intake may cause malnutrition.
Salt Restriction
Limiting sodium reduces fluid retention.
Low Saturated Fat Diet
Since lipid levels are elevated, reducing fatty foods is beneficial.
Adequate Calories
Ensures prevention of muscle loss.
Fluid Management
In severe edema, fluid intake may need monitoring.
Consultation with a dietician can help personalize the diet plan.
Prognosis
The outlook depends on the underlying cause:
- Minimal Change Disease often responds well to steroids.
- FSGS may have variable outcomes.
- Membranous nephropathy may progress slowly.
- Diabetic nephropathy may worsen if blood sugar remains uncontrolled.
Early diagnosis and consistent treatment significantly improve long-term kidney survival.
Prevention Strategies
While not all cases are preventable, risk can be minimized by:
- Strict diabetes control
- Blood pressure management
- Avoiding unnecessary use of nephrotoxic drugs
- Treating infections promptly
- Maintaining healthy body weight
- Regular kidney screening in high-risk individuals
Reference Concepts (For Further Reading)
For deeper understanding, explore related topics such as:
- Glomerular diseases
- Chronic kidney disease
- Proteinuria
- Renal biopsy interpretation
- Autoimmune kidney disorders
Conclusion
Nephrotic syndrome represents a complex kidney disorder characterized by significant protein loss, swelling, and metabolic disturbances. Though it may appear alarming, many cases respond well to early diagnosis and appropriate therapy. Identifying the underlying cause, implementing targeted treatment, maintaining dietary discipline, and ensuring regular follow-up are key pillars of successful management.
Raising awareness about symptoms like persistent swelling and frothy urine can encourage timely medical consultation and prevent long-term complications.
Frequently Asked Questions (FAQs)
What is the main cause of nephrotic syndrome?
It depends on age. In children, minimal change disease is common, while in adults, diabetes and membranous nephropathy are frequent causes.
Is nephrotic syndrome curable?
Some forms respond completely to treatment, especially minimal change disease. Others can be controlled but may not be permanently cured.
Can nephrotic syndrome lead to kidney failure?
Yes, if untreated or due to aggressive underlying diseases, it may progress to chronic kidney disease.
Why does swelling occur?
Low albumin levels reduce oncotic pressure, causing fluid to leak into tissues.
Is it hereditary?
Most cases are not inherited, but some rare genetic forms exist.
What foods should be avoided?
High-salt foods, processed foods, and excessive fatty meals should be limited.
How long does treatment last?
Treatment duration depends on the cause and response. It may last weeks to months.
Can children outgrow nephrotic syndrome?
Some children with minimal change disease achieve long-term remission.
Why are cholesterol levels high?
The liver increases lipoprotein production to compensate for protein loss.
When is kidney biopsy required?
Usually in adults or steroid-resistant cases to determine the exact type of glomerular disease.